










MultiAvail Mama
120 capsules
Full spectrum coverage with bioavailable vitamins and broad blend of minerals in their most absorbable form for optimal supplementation for pregnant women, lactating women, and women wishing to become pregnant.
The earlier supplementation begins the better as women need adequate nutrient stores to meet the demands for a growing baby and these same nutrients can support healthy fertility, metabolism, mood, and immune health. Learn more
Benefits of MultiAvail Mama
- Healthy fetal growth and development
- Metabolic support
- Hormone balance
- Mood stability
- Provides methylated Bs for brain and DNA demands
- Chelated minerals to minimize nausea and constipation
How to Take
2 capsules at 2 meals daily (4 per day, with food, yes you can take all at once but best to divide in 2 doses)
Subscription & Use Tip
Contains 120 capsules which lasts one month with typical use.
Purchase a bundle and SAVE 12%! This product is also featured in Mama To Be Bundle
Safety
- Safe with breastfeeding
- Safe during pregnancy
-
Not safe for kids
Learn more
This product also supports
Hormones and Fertility Immune and Wellness
Description
I love this unique prenatal as a foundational formula for ALL women of childbearing age, whether currently trying for a baby, pregnant, breastfeeding...or not even thinking about that right now but over age 25 and looking to maintain optimal fertility!
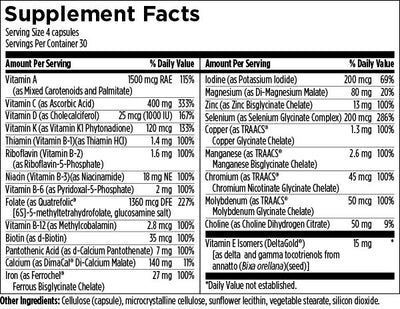
MultiAvail Mama covers all your basics with highly bioavailable nutrients and methylated Bs in place of synthetic folic acid which can drive serious drama for those that have MTHFR genetics. The minerals chosen for MultiAvail Mama are true chelates, which provide superior absorption compared to those found in standard prenatal vitamins. These minerals are dosed at levels to help achieve optimal results including calcium and magnesium for healthy bone formation, Ferrochel chelated iron as the most bioavailable iron on the market that is non-constipating and significant levels of chelated zinc to reduce risk of pre-term babies. It also features iodine to support thyroid function, growth and development and choline for cognition, liver support and beyond!
Our MultiAvail Mama contains a proprietary NatureFolate™ blend of active isomer naturally-occurring folates as a combination of L-5-MTHF and calcium folinate in place of synthetic folic acid and minerals are true chelates, which provide superior absorption compared to those found in standard prenatal vitamins.
These minerals are dosed at levels to help achieve optimal results, such as:
- Calcium and magnesium – healthy bone formation
- Ferrochel chelated iron – most bioavailable on the market, non-constipating
- Significant levels of chelated zinc – to reduce risk of pre-term babies
- Iodine – deficiency in infancy can lead to learning disabilities
- Vitamin A is provided in a 50/50 blend of preformed palmitate and mixed carotenoids with 750mcg each
The Mama-to-Be bundle combines MultiAvail Mama with EPA-DHA Extra and Restore: Baseline to provide omega-3 fatty acids for fetal brain development and regulation of inflammation, blood sugar, and blood pressure, as well as microbiome support for immune health and bowel regularity.
* These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure or prevent any disease.
Why Naturally Nourished
-
 Potency
Potency
-
 Clinical Results
Clinical Results
-
 Synergistic Formulas
Synergistic Formulas
-
 Third Party Tested
Third Party Tested
-
 Purity
Purity
Benefits
B Vitamins: required for an array of critical biochemical reactions that support healthy overall metabolism and energy production
Folate: required for DNA synthesis, healthy cellular growth and repair, and for proper development of the fetal neural tube, a structure that becomes the brain and spinal cord. The folate in MultiAvail Mama is a form of methylated folate proven to raise plasma folate levels and bypass some of the obstacles associated with synthetic folic acid, such as a genetic issues that can impair the conversion of folic acid to active folate.
Iodine & Selenium: support healthy thyroid function and synthesis of thyroid hormones. Proper thyroid hormone levels in an expectant mother help support healthy brain and neurological development in her baby.
Choline: a vitamin-like nutrient essential for proper brain development and the structure of all cell membranes
Vitamin E isomers: provided as the tocotrienol fractions of the vitamin E complex, which are more potent than the commonly used tocopherols and have different biological effects. Tocopherols are more easily obtained from a typical diet than are tocotrienols; the tocotrienols in Prenatal Pro™ augment the more readily available dietary tocopherols.
Vitamin C: provided at a level higher than the current US RDA, as the RDA was not intended to support optimum health, but rather, to prevent overt deficiency. The modern diet is generally low in vitamin C, an important antioxidant nutrient that’s also essential for a healthy immune system, collagen synthesis, and dietary iron absorption.
Chelated Minerals: The zinc, copper, manganese, molybdenum, chromium and iron in this product are provided as highly bioavailable chelates. Chelated minerals are easily absorbed and highly bioavailable because they bypass common obstacles to effective absorption, such as low stomach acid or compromised digestive function. The iron in this product will not result in constipation or GI upset, as is experienced with many conventional iron supplements.
Chromium: a trace mineral that supports proper regulation of mom’s blood sugar and insulin levels, critical for a healthy pregnancy
Q&A
I've read the recommended amount of vitamin a for pregnant women 19 years or older is 770 mcg RAE. I understand that toxicity is caused from preformed vitamin A, such as the palmitate. I know too that you can not get toxicity from taking too much of the carotenoids, which is why I would like to know the percentage of each in your product please, because your product has 1500 mcg RAE.
MultiAvail Mama has a 50/50 blend of preformed palmitate so 750mcg which is within that range of RAE with then the remaining 750mcg from mixed carotenoids.
Why use mineral chelates?
The minerals chosen for MultiAvail Mama as they offer superior absorption compared to minerals typically found in prenatal multivitamins. Zinc, manganese, molybdenum, and chromium are provided as highly bioavailable chelates. Mineral chelates do not depend on stomach acid for liberation and may be more effective for those with hypochlorhydria or other conditions that impair mineral absorption. Chelated minerals are designed to bypass obstacles to absorption and assimilation, such as food phytates, oxalates, fiber, ionic minerals or even medications that interfere with mineral absorption. Chelates are better tolerated and absorbed and are less likely to cause loose stools or other gastrointestinal discomfort. (35)
Some of the nutrients look below the necessary amounts such as magnesium, calcium, B12, and iron?
These are included at levels below the RDA because this formula is designed based on average intakes of the respective nutrients and to allow for more flexible and individualized regimens. The RDA for calcium is 1000 mg for pregnant women, while average calcium intake in women of reproductive age is 859 mg/day (35), thus the difference of 140 mg is provided by MultiAvail Mama.
If you are not consuming dairy during your pregnancy, consider adding OsteoFactors to your supplement plan.
The same rationale was applied to magnesium: the RDA is 360 mg but average dietary intake is estimated to be 281mg. (35) The 80 mg of magnesium provided by MultiAvail Mama makes up for this shortfall.
If you deal with muscle cramps, hypertension, headaches, or constipation, you may benefit from adding Relax and Regulate to your supplement plan.
Chelated Iron: (as Ferrochel® ferrous bisglycinate chelate) was chosen due to its high bioavailability and tolerability. The chelated form will not result in the constipation commonly induced by iron supplementation.
Average intake of iron by women of reproductive age in the US is 14 mg/day with a range of 7.3–22.3 mg/day. (35) The value of 13 mg of iron chosen for this formula was derived as the difference between the RDA (27 mg) and this estimated average intake. It also ensures that the upper range of iron intake plus the amount in MultiAvail Mama falls within a safe margin of 45 mg (the upper tolerable level of iron intake).
Well-balanced diets, such as my Anti-Anxiety Diet or whole food keto approach provides iron in the range of 17–22 mg/day. One study found that supplementation with iron bisglycinate chelate resulted in double the absorption compared to ferrous sulfate when taken with breakfast. This form of iron partially prevented the inhibitory effect of phytates, had low interactions with food, and showed high solubility in aqueous solutions even at a pH 6.36
Many clients including myself benefit from an additional b-complex which can support energy and mood stability throughout pregnancy especially for those under high stress levels. Consider adding B-complex and/or B-12 Boost.
Research
Iodine is a trace element essential for synthesis of the thyroid hormones, triiodothyronine and thyroxine. These hormones play a vital role in the early growth and development stages of most organs, especially the brain.
During pregnancy sufficient quantities of iodine are required to prevent the appearance of hypothyroidism, trophoblastic and embryonic or fetal disorders, neonatal and maternal hypothyroidism, and permanent sequelae in infants. Thyroid hormone receptors and iodothyronine deiodinases are present in placenta and central nervous tissue of the fetus.
Faustino R. Pérez-lópez (2007) Iodine and thyroid hormones during pregnancy and postpartum, Gynecological Endocrinology, 23:7, 414-428, DOI: 10.1080/09513590701464092
Folate: provided as Quatrefolic®, a glucosamine salt 5-MTHF form of folate proven to dissociate reliably before absorption and raise plasma folate levels. (14) This form of 5-MTHF is likely more bioavailable than naturally occurring folates because those are covalently bonded to polyglutamate chains. The Quatrefolic® form of folate was shown to be 1.12 times and 9.7 times more bioavailable than the calcium salt of 5-MTHF and folic acid, respectively.(15) Research showed that plasma folate levels were brought above the desired level of 50 nM more quickly with 5-MTHF than with folic acid supplementation. This effect is critical because women with low folate status may first become aware of their pregnancy when fetal cell proliferation and differentiation develop at a fast pace and may already have been negatively impacted by folate deficiency.16
Folic acid is no longer considered an adequate source of folate for the following reasons:
(a) genetic polymorphisms of folate metabolism are common and are responsible for a 35-70% reduced conversion
of folic acid to the biological active form, 5-MTHF14,17
(b) unmetabolized folic acid has been detected in umbilical cord blood at birth18
(c) synthetic folic acid (derived from fortified foods and/or supplements) may increase the risk of various cancers, reduce natural killer (NK) cell activity, and may have other detrimental
effects (17,19)
(d) human physiology is adapted to natural folates; folic acid is not a naturally occurring molecule
and has a distinct pathway of cell entry and different metabolic transformations compared to natural folates.
These differences may be responsible for the detrimental effects associated with folic acid.(17,20) Adequate folate status was also shown to be relevant to risk of pre-eclampsia, which was reduced by supplementation with 5-MTHF.21 This may be due to improvement of nitric oxide levels, which would support healthy blood pressure. A study looked at the effect of supplementing pregnant women with 5-MTHF alone, folic acid alone, or 5-MTHF and folic acid combined, on their children’s mental abilities at age 8.5 years. Results showed that progeny of mothers supplemented with 5-MTHF had “higher activation of the midcingulate cortex, indicating that early nutrition influences the functionality of specific brain areas involved in executive functions.” (22)
1. Lucock MD, Martin CE, Yates ZR, Veysey M. Diet and our genetic legacy in the recent anthropocene: a
Darwinian perspective to nutritional health. J Evid Based Complementary Altern Med. 2014 Jan;19(1):68-
83. doi: 10.1177/2156587213503345. Review. PubMed PMID: 24647381.
2. Kuipers RS, Joordens JC, Muskiet FA. A multidisciplinary reconstruction of Palaeolithic nutrition
that holds promise for the prevention and treatment of diseases of civilization. Nutr Res Rev. 2012
Jun;25(1):96-129. doi: 10.1017/S0954422412000017. Review. PubMed PMID: 22894943.
3. Jew S, Abu Mweis SS, Jones PJ. Evolution of the human diet: linking our ancestral diet to modern
functional foods as a means of chronic disease prevention. J Med Food. 2009 Oct;12(5):925-34. doi:
10.1089/jmf.2008.0268. Review. PubMed PMID: 19857053.
4. Cordain L., The Nutritional Characteristics of a Contemporary Diet Based Upon Paleolithic Food Groups.,
JANA Vol. 5, No. 3, 2002., 14-24.
5. Fenech M. Micronutrients and genomic stability: a new paradigm for recommended dietary allowances
(RDAs). Food Chem Toxicol. 2002 Aug;40(8):1113-7. Review. PubMed PMID: 12067572.
6. Fenech M, Ferguson LR. Vitamins/minerals and genomic stability in humans. Mutat Res. 2001 Apr
18;475(1- 2):1-6. PubMed PMID: 11295148.
7. Fenech M. Nutritional treatment of genome instability: a paradigm shift in disease prevention and in
the setting of recommended dietary allowances. Nutr Res Rev. 2003 Jun;16(1):109-22. doi: 10.1079/
NRR200359. PubMed PMID: 19079941.
8. Fenech M. Folate (vitamin B9) and vitamin B12 and their function in the maintenance of nuclear and
mitochondrial genome integrity. Mutat Res. 2012 May 1;733(1-2):21-33. doi: 10.1016/j.mrfmmm.2011.11.003.
Review. PubMed PMID: 22093367.
9. Summers CM, Mitchell LE, Stanislawska-Sachadyn A, Baido SF, Blair IA, Von Feldt JM, Whitehead AS
Genetic and lifestyle variables associated with homocysteine concentrations and the distribution of folate
derivatives in healthy premenopausal women. Birth Defects Res A Clin Mol Teratol. 2010 Aug;88(8):679-
88. doi: 10.1002/bdra.20683. PubMed PMID: 20544798; PubMed Central PMCID: PMC4051228.
10. 5-methyltetrahydrofolate. Monograph. Altern Med Rev. 2006 Dec;11(4):330-7.
11. Mazza A, Cicero AF, Ramazzina E, Lenti S, Schiavon L, Casiglia E, Gussoni G. Nutraceutical approaches
to homocysteine lowering in hypertensive subjects at low cardiovascular risk: a multicenter, randomized
clinical trial. J Biol Regul Homeost Agents. 2016 Jul-Sep;30(3):921-927. PubMed PMID: 27655522.
12. Deshmukh US, Joglekar CV, Lubree HG, Ramdas LV, Bhat DS, Naik SS, Hardikar PS, Raut DA, Konde TB,
Wills AK, Jackson AA, Refsum H, Nanivadekar AS, Fall CH, Yajnik CS. Effect of physiological doses of oral
vitamin B12 on plasma homocysteine: a randomized, placebo-controlled, double-blind trial in India. Eur J
Clin Nutr. 2010 May;64(5):495-502. doi: 10.1038/ejcn.2010.15. PubMed PMID: 20216560; PubMed Central
PMCID: PMC2865445.
13. Servy EJ, Jacquesson-Fournols L, Cohen M, Menezo YJR. MTHFR isoform carriers. 5-MTHF (5-methyl
tetrahydrofolate) vs folic acid: a key to pregnancy outcome: a case series. J Assist Reprod Genet. 2018
Aug;35(8):1431-1435. doi: 10.1007/s10815-018-1225-2. PubMed PMID: 29882091; PubMed Centra PMCID:
PMC6086798.
14. White paper on 5-MTHF (Quatrefolic), by Gnosis. https://www.quatrefolic.com/whitepaper.php
15. Miraglia N, Agostinetto M, Bianchi D, Valoti E. Enhanced oral bioavailability of a novel folate salt:
comparison with folic acid and a calcium folate salt in a pharmacokinetic study in rats. Minerva Ginecol.
2016 Apr;68(2):99-105. PubMed PMID: 27008238.
16. Bailey SW, Ayling JE. The pharmacokinetic advantage of 5-methyltetrahydrofolate for minimization of
the risk for birth defects. Sci Rep. 2018 Mar 6;8(1):4096. doi: 10.1038/s41598-018-22191-2. PubMed PMID:
29511242; PubMed Central PMCID: PMC5840174.
17. Tam C, O’Connor D, Koren G. Circulating unmetabolized folic Acid: relationship to folate status and
effect of supplementation. Obstet Gynecol Int. 2012;2012:485179. doi: 10.1155/2012/485179. PubMed
PMID:22529856.
Prenatal Pro™
18. Obeid R, Kasoha M, Kirsch SH, Munz W, Herrmann W. Concentrations of unmetabolized folic acid and
primary folate forms in pregnant women at delivery and in umbilical cord blood. Am J Clin Nutr. 2010
Dec;92(6):1416-22. doi: 10.3945/ajcn.2010.29361. PubMed PMID: 20844072.
19. Sauer J, Mason JB, Choi SW. Too much folate: a risk factor for cancer and cardiovascular disease? Curr
Opin Clin Nutr Metab Care. 2009 Jan;12(1):30-6. doi: 10.1097/MCO.0b013e32831cec62. Review. PubMed
PMID: 19057184; PubMed Central PMCID: PMC2790187.
20. Prinz-Langenohl R, Brämswig S, Tobolski O, Smulders YM, Smith DE, Finglas PM, Pietrzik K. [6S]-
5- methyltetrahydrofolate increases plasma folate more effectively than folic acid in women with
the homozygous or wild-type 677C-->Tpolymorphism of methylenetetrahydrofolate reductase. Br J
Pharmacol. 2009 Dec;158(8):2014-21. doi: 10.1111/j.1476-5381.2009.00492.x. PubMed PMID:19917061;
PubMed Central PMCID: PMC2807663.
21. Saccone G, Sarno L, Roman A, Donadono V, Maruotti GM, Martinelli P. 5-Methyl-tetrahydrofolate
in prevention of recurrent preeclampsia. J Matern Fetal Neonatal Med. 2016 Mar;29(6):916-20. doi:
10.3109/14767058.2015.1023189. PubMed PMID: 25777577.
22. Catena A, Muñoz-Machicao JA, Torres-Espínola FJ, Martínez-Zaldívar C, Diaz-Piedra C, Gil A, Haile G,
Györei E, Molloy AM, Decsi T, Koletzko B, Campoy C. Folate and long-chain polyunsaturated fatty acid
supplementation during pregnancy has long-term effects on the attention system of 8.5-y-old offspring:
a randomized controlled trial. Am J Clin Nutr. 2016 Jan;103(1):115-27. doi: 10.3945/ajcn.115.109108. PubMed
PMID: 26561619.
23. Abdul Niefaizal Abdul Hammid, Junedah Sanusi, Huzwah Khaza’ai, Mohd Sokhini, Abd Mutalib, Zaleha
Abdullah Mahdy, Maria Mahmood, Hartini Md Yon. IPregnancy Outcome in Rats Following Exposure to
A Palm Vitamin E. International Journal of Basic and Applied Science, Vol. 03, No. 02, October 2014, pp.
143-153.
24. Paumgartten FJ, De-Carvalho RR, Araujo IB, Pinto FM, Borges OO, Souza CA, Kuriyama SN. Evaluation of
the developmental toxicity of annatto in the rat. Food Chem Toxicol. 2002 Nov;40(11):1595-601. PubMed
PMID: 12176086.
25. Mohd Mutalip SS, Rajikin MH, Ab Rahim S, Mohamed Noor Khan N. Annatto (Bixa orellana) δ-TCT
Supplementation Protection against Embryonic Malformations through Alterations in PI3K/Akt-Cyclin D1
Pathway. Biomolecules. 2019 Jan 10;9(1). pii: E19. doi: 10.3390/biom9010019. PubMed PMID: 30634632;
PubMed Central PMCID: PMC6358786.
26. Nagapan G, Meng Goh Y, Shameha Abdul Razak I, Nesaretnam K, Ebrahimi M. The effects of prenatal
and early postnatal tocotrienol-rich fraction supplementation on cognitive function development in male
offspring rats. BMC Neurosci. 2013 Jul 31;14:77. doi: 10.1186/1471-2202-14-77. PubMed PMID: 23902378;
PubMed Central PMCID: PMC3750608.
27. Abd Aziz NAA, Chatterjee A, Chatterjee R, Durairajanayagam D. Tocotrienol-rich fraction
supplementation prevents foetal loss in females mated with corticosterone-treated male Sprague-Dawley
rats. Andrologia. 2019 Apr;51(3):e13199. doi: 10.1111/and.13199. PubMed PMID: 30461035
28. Kamsani YS, Rajikin MH, Mohamed Nor Khan NA, Abdul Satar N, Chatterjee A. Nicotine-induced
cessation of embryonic development is reversed by γ-tocotrienol in mice. Med Sci Monit Basic Res.
2013 Mar 6;19:87-92. doi: 10.12659/MSMBR.883822. PubMed PMID: 23462735; PubMed Central PMCID:
PMC3638657.
29. Rajikin, M.H.; Nor-Ashikin, M.N.K.; Nuraliza, A.S. Tocotrienol improves the quality of impaired mouse
embryos induced by corticosterone. In Proceedings of the Symposium on Humanities, Science and
Engineering Research (SHUSER2012), Kuala Lumpur, Malaysia, 24–27 June 2012; pp. 135–138.
30. Nur Azlina MF, Nafeeza MI. Tocotrienol and alpha-tocopherol reduce corticosterone and noradrenalin
levels in rats exposed to restraint stress. Pharmazie. 2008 Dec;63(12):890-2. PubMed PMID: 19177905.
31. Roy S, Lado BH, Khanna S, Sen CK. Vitamin E sensitive genes in the developing rat fetal brain: a highdensity oligonucleotide microarray analysis. FEBS Lett. 2002 Oct 23;530(1-3):17-23. PubMed PMID:
12387859; PubMed Central PMCID: PMC1832147.
32. C. Paul. Vitamin K-Chapter 136. Textbook of Natural Medicine (4th edition), editors Michal Murray, Joseph
Pizzorno ISBN-13: 9781437723335 Publisher: Elsevier Health Sciences: 9/28/2012.
33. Abdullah M, Jamil RT, Attia FN. Vitamin C (Ascorbic Acid). 2019 Jun 3. StatPearls Publishing; 2019 Jan.
Available from http://www.ncbi.nlm.nih.gov/books/NBK499877/PubMed PMID: 29763052.
34. Ashmead, H.D., Graff, D.J., Ashmead, H.H. (1985): Intestinal Absorption of Metal Ions and Chelates.
Charles C. Thomas, Springfield, Illinois.
35. NHANES (National Health and Nutrition Examination Survey) 2001-2002. www.CDC.gov.
36. L ayrisse M, García-Casal MN, Solano L, Barón MA, Arguello F, Llovera D, Ramírez J, Leets I, Tropper
E. Iron bioavailability in humans from breakfasts enriched with iron bis-glycine chelate, phytates and
polyphenols. J Nutr. 2000 Sep;130(9):2195-9. PubMed PMID: 10958812.
37. Roohani N, Hurrell R, Kelishadi R, Schulin R. Zinc and its importance for human health: An integrative
review. J Res Med Sci. 2013 Feb;18(2):144-57. PubMed PMID: 23914218; PubMed Central PMCID:
PMC3724376.
38. Anderson RA. Chromium as an essential nutrient for humans. Regul Toxicol Pharmacol 1997; 26:S35-41.
39. Lamson DW, Plaza SM. The safety and efficacy of high-dose chromium. Altern Med Rev. 2002
Jun;7(3):218-35. Review. PubMed PMID: 12126463.
40. Hotz CS, Fitzpatrick DW, Trick KD, L'Abbe MR. Dietary Iodine and selenium interact to affect thyroid
hormone metabolism of rats. J Nutr 1997; 127:1214-8.
41. Arthur JR, Nicol F, Beckett GJ. The role of selenium in thyroid hormone metabolism and effects of
selenium deficiency on thyroid hormone and iodine metabolism. Biol Trace Elem Res 1992; 33:37-42.
42. BD Tiwari, et al. Learning disabilities and poor motivation to achieve due to prolonged iodine deficiency.
American Journal of Clinical Nutrition, Vol 63, 782-786, 1996.
43. Pérez-López FR. Iodine and thyroid hormones during pregnancy and postpartum. Gynecol Endocrinol.
2007 Jul;23 (7): 414-28
44. LaFranchi SH, Haddow JE, Hollowell JG. Is thyroid inadequacy during gestation a risk factor for adverse
pregnancy and developmental outcomes? Thyroid. 2005 Jan;15(1):60-71.
45. Li Y, et al. Abnormalities of maternal thyroid function during pregnancy affect neuropsychological
development of their children at 25-30 months. Clin Endocrinol (Oxf). 2010 Jun;72(6):825-9.
46. Glinoer D. Potential consequences of maternal hypothyroidism on the offspring: evidence and
implications. Horm Res. 2001;55(3):109-14.
47. Caldwell KL, Pan Y, Mortensen ME, Makhmudov A, Merrill L, Moye J. Iodine Status in Pregnant Women
in the National Children’s Study and in U.S. Women (15–44 Years), National Health and Nutrition
Examination Survey 2005–2010. Thyroid. 2013;23(8):927-937.
48. Shichiri M, Takanezawa Y, Uchida K, Tamai H, Arai H. Protection of cerebellar granule cells by tocopherols
and tocotrienols against methylmercury toxicity. Brain Res. 2007 Nov 28;1182:106-15. PubMed PMID:
17949699.
MultiAvail Mama
120 capsules